Posts Tagged: health
concentric circle origami
-
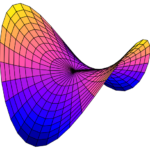
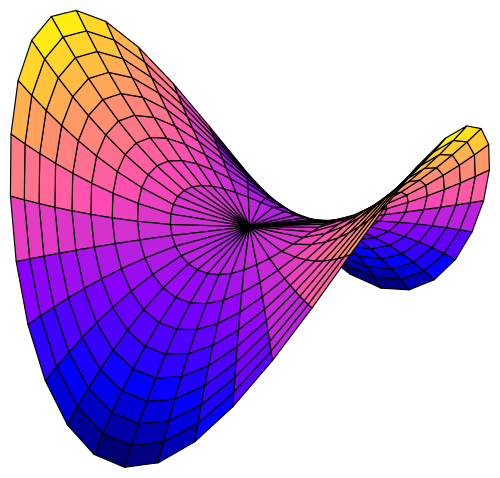
- hyperbolic paraboloid (hypar)
-

- scored vinyl

-

- creasing the concentric circles

-

- …and more

-

- starts to flatten out as you get close

-

- but eventually

-

- it begins to ‘pop’

-

- at that point it can be looped through itself

-

- and weird things happen

-

- ”flat-ish“ hypar sphere intersection

-
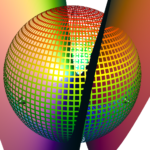
- “extreme” hypar sphere intersection

-
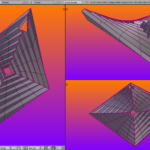
- a square version to compare to other physical models
Brief Thoughts on The Brain
So I’ve been thinking lately about some different ways to view the brain, and causality, and I think there is an unsettled question.
I recall reading about a study of London cab drivers that suggested the part of the brain that stores directions was proportionally bigger in the brains of cab drivers who had been working longer, and I think the natural conclusion was that like muscles being exercised becoming stronger and healthier, exercising the “directions” part of the brain made it bigger and stronger as well. Which would make a lot of sense. But there is an alternative explanation, which would be that some people are born with bigger “directions” parts of the brains, and those people naturally become more long-term cab drivers. This doesn’t fit quite as well if there is correlation between the length of time they’ve been a cab driver and the size of that brain part, because you’d expect to find young cab drivers with varying sizes, and the ones with the biggest being the ones you’d expect to last the longest. I’m not sure what the research found, I should probably be looking it up.
The reason I bring this up is that this second view tends to be how we view mental illnesses, as problems with the brain that cannot be reversed through “exercise”. I find this particularly concerning with diagnosing children with mental illnesses, as their brains are still developing and I think we don’t yet know enough to safely say a developing brain truly has a problem (in most instances), or if its merely a stage in the maturing process. I watched a documentary on medicating children for mental illness a few years ago on Netflix and was astounded by the fact that some children were diagnosed as young as five, put on drugs that affected their brain chemistry, and believed they could never function without them. I’m not saying that maybe isn’t true in some cases, but I think it would take some pretty hefty evidence to convince me.
I’ve also been thinking for quite a while now that if we truly understood mental illness, we’d be able to cure it reliably, which we cannot, and that’s an indicator we don’t yet understand the problem. PTSD for example is cured in some people, but it seems that most that suffer from it continue to suffer from it indefinitely, suggesting we don’t really know how to cure it. As opposed to traditional illnesses like bacterial infections or bone fractures.
Anyway, I’m not necessarily siding with one view or the other, just noting that there are two competing views on how the brain works, and while I want to lean towards the one, I think we still need more evidence to really know which. I suppose there is the possibility that both are true to varying degrees, but teasing apart the strength of each one would still be ahead of us as well. I guess just keeping in mind the fact that “practice makes perfect” is well established, and remembering that our brains are plastic and nothing is set in stone, are good things to know when dealing with mental illnesses.
Home Again for Now
So I was released on Wednesday, the 19th, and have been home the last two days. My ANC was 320 Wednesday morning, which was really discouraging, since it had been 400 the day before and they had told me if it remained at 400 I could go home. So I spent a few hours thinking I’d be stuck there at least a few more days. But then later in the day they told me that they don’t think anything weird is happening, my numbers are just kind of bouncing around a bit, which is fairly typical, and since I’ve been through all this repeatedly they trust me to look for signs of infection and seek medical help if I have any complications. And since I was just waiting around to recover, I might as well do that in the comfort of my own home. So I got to go home! They wanted to give me a blood transfusion before leaving, cause my hemoglobin was like 7 something, and outside the hospital they want it to be at least 8, so they did a transfusion and then another blood count and it was really good news, my ANC had gone up to 370, my hemoglobin was 9 I think(?) and my platelets had ticked up a little bit from the morning as well.
They did a bone marrow biopsy on Monday, but it was kind of too early, there were blast cells, which could potentially be leukemia cells, but they may also just be normal healthy cells that haven’t matured yet. So they’ll want to perform another biopsy sometime soon, this week probably, and if that looks good I should be all ready to start the transplant process at MGH. On Monday I’ll go in for a more routine checkup to make sure the numbers are looking good, and then my hope is, if all that checks out, we can go into the transplant process as soon as is possible. I’m nervous about it, but I’m more nervous that any waiting is giving the leukemia cells more time to regrow.
Someone contacted me about reworking the octopus to be smaller. I’ve wanted to redesign a lot of things about it for a long time, so I might actually try to do that finally. It has me digging through old project files trying to decide how to go about it. I had also begun a cuttlefish model not long ago, so I might just start with that instead. I think I should learn about rigging the model up this time, so I can more easily rearrange the legs in the future.
Reinduction
So I was re-admitted to the hospital on Monday for another round of induction chemotherapy, it consisted of two new (to me) drugs, each administered once a day for five days, so last night was my last dose of each. Now I’ll be hanging around for the next three weeks, waiting for my counts to drop down and then rebound, after which I’ll head to Boston for the transplant process.
So far it’s been pretty easy going, I’ve been walking a lot, which is both good for my health, and allows me to avoid painful shots in the stomach that they give to most patients to help avoid clots from forming in the calves. Today they disconnected me entirely so I can walk around without pushing the pole of fluids with me, which is nice too. It could be a little rough over the next two weeks, I’ll probably need some transfusions as my blood and platelets die off temporarily, though it shouldn’t really be anything I haven’t already seen in the past.
I have a lot to work on, and plenty of distractions. I should make more of an effort to try out some things, and I also have to delete photos to make room on my computer and my phone. That’s all for now!
An Upcoming Third Round
My updates have been infrequent lately, I suppose because I don’t think there has been much to report.
I had a folllowup appointment yesterday, my platelets and ANC have recovered well, which is nice, but my hemoglobin remains low, which just means I tire easy, and get a little dizzy when I first stand up, or take too many deep breaths in a row.
On Friday, July 1st, I met with the transplant doctor and her team, in Boston, to begin learning about the entire transplant process. She figured it’d begin in about six weeks, after they’ve checked me out thoroughly and decided I’m ready. I need to get a dentist appointment to make sure my mouth is in good shape before we begin. And they don’t really like going more than I think she said 8 weeks between consolidation chemotherapies and the transplant process, so I’ll be back at Dartmouth Hitchcock next week, probably Thursday, maybe Wednesday, for another round of consolidation. Mostly the consolidation chemotherapies have been pretty tolerable, though the complications afterwards — the nosebleed the first time and the fever the second time — resulted in a lot of unpleasant experiences. It feels like each one is teaching me to be more cautious about some aspect following the chemotherapy. After the nosebleed we took some extra precautions to keep my nose clean and less likely to bleed, now I’m going to take further precautions in the weeks my ANC bottoms out, make sure to wear a mask anytime I’m in public and so on.
The transplant process is going to be much longer, and tougher, than what I’ve been doing for consolidation. The chemotherapy will be much more potent, as it’s intention won’t just be to keep my immune cells somewhat suppressed, but to actual wipe the immune cells out more completely, in preparation for a donor immune system to take hold. Typically this process requires three or four weeks of hospitalization, after they wipe out the immune system, receiving the donor immune system is basically like a blood transfusion. Then hopefully it grows into my bone marrow, and begins to provide me with a new immune system. There is some concern about the new donated immune system attacking me as if I were a foreign invader, that’s called graft-vs-host-disease, or GvHD, it’s similar to the kinds of rejection they worry about with organ transplants, only in that case it is the recipient’s immune system attacking the donated organ, in my case it’d be the donated organ attacking other stuff. The main targets tend to be the skin, the lungs, and the liver, and the doctors will provide some treatments if I show signs of those problems. I saw a video a while back on bethematch.org where people who’ve gone through this said it’s actually good to have some minor symptoms of GvHD, because it means the donated immune system is working and taking hold, and there is even an effect called graft-versus-tumor, where the new immune system attacks the old one and helps kill off any remaining cancerous blast cells. There is about a 10-15% chance that the process kills me, and about a 50-60% chance that it cures me. I didn’t ask, but I think that remaining 25-40% chance that I survive the donation process but the leukemia returns, at that point we start discussing other treatment options, I suspect probably clinical trials because I think this is the only real standard way to treat aggressive leukemias at the moment.
So that’s where my adventures in health are at the moment. Mostly a high degree of uncertainty, some unpleasant future stuff, but I’m glad to be born at a time when we know at least somewhat how to deal with this problem, and not decades or centuries ago when it would have just killled me right away.
Other than that I’ve been skipping around between projects, trying to focus on some experimental camera app idea. I got a lot of photos of the Fourth of July fireworks with my app trippygram, which I’ve been sharing on Instagram. I also made a snowflake gallery, though it’s terribly mismanaged, I need to delete about a hundred photos probably. At least the ones that are very similar to one another. I got tired of sorting through them trying to decide which was better.
Another Nadir
So I had a checkup today, platelets and hemoglobin were pretty low (14 and 8.3 respectively) so they gave me transfusions for each of them. My ANC was low, 740, but not neutropenic, so probably I’m still on the way down, and gonna bottom out some time in the next several days. I’ll be avoiding public for a while, again, which is all expected.
Programming-wise I’ve been learning how to incorporate Objective C code in with the Swift code I work in by using a bridging header. Expanding my understanding of how to program feels really good, and should pay off as better software in the end. This should make it easier for me to get permission from the user to use the camera, and store photos, and maybe resolve some of the issues I had originally with it not granting permission the first time — which I think I solved, but was told there were better solutions still. Also it should let me handle metadata finally, which I’ve been struggling with. I can get the original metadata when the photo is taken, but never figured out how to save it with the resulting photo. I’d also like to add a “made with” tag in the metadata, so maybe I can do that soon too. Then I may need to have an actual privacy policy…
I made a tips & tricks page a while back, because I know I’ve learned a lot over the years about what works best in certain situations, and it would help if I could share that with other people. I should probably try to streamline that page as much as possible, and then incorporate it into some kind of help/tutorial/introduction to the app. So any feedback on that page would be greatly appreciated!
I haven’t worked on zeeify lately, and am going to shift it to spectrify, which will take a series of photos and use a cheap method of edge detection and then use the same kind of colorization schemes trippygram uses — mostly because this will all be easier to do and I’m curious what the results will look like. Plus if I’m going to colorize them, it won’t matter so much that I’ve used a cheaper method to cut out the sharp stuff.
And all that should keep me plenty occuppied for a while. I was thinking recently I should apply to be a substitute teacher, but I feel like I need to wait until my health situation is more stable, maybe after the transplant process, if that all goes well, maybe as I recover I’ll be able to do something like substitute teaching. Guess I’ll wait and see!
Not Much to Report
So I’ve been re-admitted, as planned, probably until Saturday evening. My platelet count was 70, which wasn’t much higher than last week, and lower than the 100 they wanted for readmission, but they decided to wave it to get going on this round.
It’s all very familiar. Seeing all the nurses and doctors I’ve met. Eyedrops that make my food taste bad, but protect my eyes from the chemotherapy drug. Going for walks to avoid getting a painful shot of Lovonox in my stomach. Hickuping coming and going periodically. Feels very routine at this point.
But this should be the last round of consolidation chemotherapy before they try a bone marrow transplant. They never found a good match, so they’ll do a partial match transplant instead, which isn’t done here at Dartmouth, but rather down in Boston, Mass General I think.
The first two doses have been administered, they each last three hours, with twelve hours between them, and then thirty hours between each pair of doses. So two down, six to go.
Other than that I’m not sure what to say. I was working more on some software again before coming back to the hospital, and plan on working on it more while I’m here.
Another Consolidation
So after the long weekend, on Tuesday, I’ll be re-admitted for another round of consolidation chemotherapy, for probably five or six days. Typically they do two rounds of consolidation and then a transplant, which involves another month in the hospital. They haven’t found a great match, so at the moment it looks like they’ll try a partial match, in which case they won’t do it at Dartmouth Hitchcock in Lebanon, but somewhere in Boston, I guess probably Mass General hospital.
The risks are greater with a partial match, but it’s still successful for some people, and because of the specific cause in my case there is a high likelihood of relapse without a tranpslant, so the potential benefit of a transplant is enormous and symmetrical to the risk of no transplant. I don’t know a whole lot about the transplant process yet, and I may be repeating myself some here, but the basic idea is that my bone marrow has a mutation (inversion on chromosome 3), which caused it to produce white blood cells that didn’t mature. Normally the bone marrow produces white blood cells that mature into different kinds of cells that do different things, in my case the cells aren’t maturing and the young undifferentiated cells began to crowd out the mature white blood cells and the red blood cells that carry oxygen. So we kill off all the immature cells with the chemotherapy and then take someone else’s bone marrow, and ideally, it grows into my bones and produces healthy blood cells.
The search is for Human Leukocite Antigen (HLA) matching, which is the fancy technical term for the proteins on the outside of cells that the immune system uses to identify which cells are part of the body, and which are foreign invaders. The better the match, the less of a likelihood that the donated immune system attacks the rest of my body as foreign, which is known as graft-vs-host disease (GVHD). It’s similar to other organ donation concerns, except normally they’re concerned that the recipient’s immune system will attack the donor organ, in this case the donation is the immune system itself, so the concern is more about it attacking everything else. The other major concern seems to be that the donated immune system takes hold in my bones. Apparently having some symptoms of GVHD is actually reassuring because it indicates that the donated immune system is in fact doing it’s job, and it could even potentially target any remaining blast cells (cancerous immature immune cells).
The difficulty in finding a good match is because they’re hoping to match ten antigens (ideally, based on research about which donations have been most successful), two known as HLA-A, two as -B, two as -C, two as -DRB1, and two as HLA-DQ. The criteria seem to grow more specific as we collect more information about the genome and which transplants are more successful, so I think they used to look for six markers, then eight, now ten. To better understand the odds, I looked up HLA markers on wikipedia, and found there are 2,884 HLA-A alleles, 3,589 HLA-B alleles, and 2,375 HLA-C alleles; there are 1,540 HLA-DRB1 alleles, and theoretically maybe 34,528 possible combinations of HLA-DQ type alleles. (Alleles are variations of a given gene.)
A very simplistic (and inaccurate) estimate of the relevant variability here would be to simply multiply all these numbers together, but in reality not all these combinations are likely to occur, I’m sure there are strong correlations for certain sets of alleles across markers, but it’s still helpful to get an idea of why matching is so difficult. It’s interesting that there is such tremendous genetic variation in this case because our ancestors seem to have gone through some genetic bottlenecks in the past that reduced our variation in a lot of ways. But there seems to be evidence that humans actually seek out genetic variability in mate selection — there is an obvious benefit to increased genetic diversity in offspring, that’s the whole reason sexual reproduction exists, and in retrospect it’s not surprising that that benefit would be compounded for immune systems. In other words, the reason we have such great diversity in our immune systems is probably that we’re actively seeking mates to maximize the diversity — for the last 150,000 years we’ve probably been actively maximizing the diversity of our immune systems. (This was all a digression I inserted after writing the next part, and I only mention that because I don’t feel like editing together something better than the non-sequitar below.)
I’m feeling pretty close to normal, a bit weaker than I used to be, and I still get a little light headed at times, when transitioning from crouched down to standing up, but I’m mostly feeling pretty much like I used to.
I went to a beach in Maine on Thursday with Justine, which was fun. I had weird feelings about being in public, I guess because of how my immune system was still a little weak, which makes me feel a little cautious about being around lots of people. Last night I went to a baseball game and felt a little more comfortable about that problem. It’s weird feeling normal but also knowing that a minor infectious disease could be life-threatening. I also put sunscreen all over the top of my head, which was a new experience for me.
I haven’t really made any progress on zeeify lately, stuck on a bug, but I’m beginning to think I should just not worry about the final quality of the image at the moment and look into making another fun color-driven app. Maybe that should be spectrify. I dunno. But it’s good to be working on something.
That’s all for now!
Numbers Update
I had an appointment to get my blood checked yesterday, and I didn’t need any transfusions, which was nice. I made some good progress on the puzzle in the waiting room. I go back Thursday, and then have it done up in Lebanon next Monday, which if everything is doing well I’ll get re-admitted for another week and do this all over again! I’m feeling okay, kinda tired still, but by the amount expected for my hemoglobin I suppose.
My ANC, the sort of first line of defense white blood cells was 0.17, on Thusday it was 0.01, and on Wednesday I had zero detectable white blood cells so the ANC wasn’t even measured. Normal is 1.4-7.7, I don’t know exactly what would be enough to be re-admitted Wednesday but it seems like theres a good chance I will be.
Other than that I guess I should be drinking more water.
Bottoming Out
So I had appointments Wednesday and Thursday, Wednesday my white blood cell count was 0 — neutrophils are a type of white blood cell, so they were 0 as well. Thursday they were 0.01, so maybe they’re starting to bounce back, my next check is on Monday so I’m staying in this weekend and wearing a mask when I have to be in public. I had another blood transfusion on Thursday but my platelets (28) were still well above the transfusion threshold (20), so that was reassuring. A doctor told me usually it bottoms out in days 10-14, but I was on day 16 Wednesday, and that wasn’t surprising because the first couple rounds of chemotherapy had really done a number on my immune system. So I’ve been unconcerned about it.
Getting prescriptions transferred and refilled has been a lot more annoying than I would have otherwise expected, but I think I have it all straightened out finally.
Longer term my next appointment with the doctors is Monday the 23rd, and if my numbers look good they’ll admit me for another round of consolidation chemotherapy — so I get to look forward to repeating all this again in the next few weeks. After that I guess we’ll be looking at how to get someone else’s immune cells into me, but so far the donor search hasn’t found any 10 of 10 matches. If they can’t find any match I guess they’ll do a partial match, which carries a greater risk that the donated immune system could mistake me for a foreign invader and attack me. I haven’t asked what we do if that happens, I guess I’ll ask as we get closer to that.
In other news I’m working on a toy idea inspired by curved crease origami, and just ordered a sample of a flexible material to see how much the idea might work out, so I’m kind of excited about that.
![]()
![]()
![]()
![]()